Scoliosis and kyphosis treatment: can spinal curves be corrected?
Kyphosis and scoliosis come in two very different forms — flexible postural curves that respond well to care, and structural curves that are managed, not cured. The honest difference, and what to do about each.
Every spine has curves, and that is exactly how it should be. Viewed from the side, a healthy spine gently waves — a soft inward curve at the neck and low back, a soft outward curve through the upper back. Those curves are shock absorbers. The trouble starts only when a curve deepens too far, or when the spine begins to twist sideways where it shouldn't. That is the territory of kyphosis and scoliosis.
Anatomy made simple
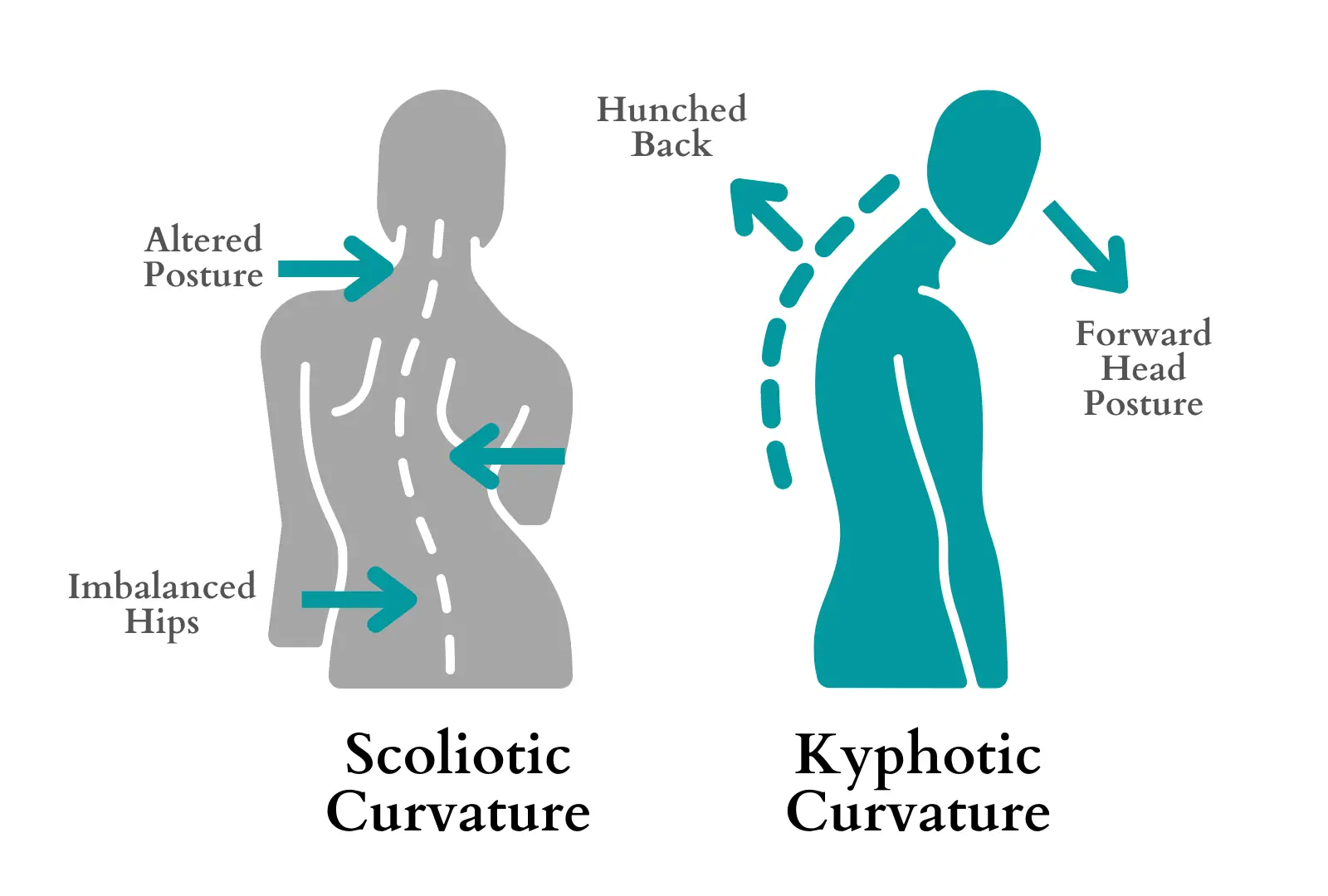
The two conditions describe curves in different planes. Kyphosis is an exaggerated outward curve of the upper back — the rounded, hunched-forward posture that drags the head in front of the shoulders. Scoliosis is a sideways curve, often with a rotational twist, that bends the spine into a subtle C or S shape when viewed from behind.
Some curvature is structural — built into the bones themselves, as in adolescent scoliosis or the wedge-shaped vertebrae of certain kyphosis. A great deal of what we see in adults, though, is postural: curves driven and reinforced by how we hold ourselves, by hours of forward-flexed sitting, and by muscle imbalances that pull the spine out of its neutral stack.
That distinction matters enormously. Structural curves are managed and monitored; postural and flexible curves often have real room to improve with the right work. Mayo Clinic outlines how clinicians distinguish and track them over time.
How it connects to the Pain Locator
Postural curvature changes ripple across several regions of the Pain Locator, because a spine that is out of its neutral stack forces muscles to work overtime to hold you up. The common markers:
- Mid-back aching — the upper-back muscles fatigue from fighting a deepening forward curve
- Forward head carriage — the head drifts ahead of the shoulders, multiplying the load on the neck
- Uneven hip or shoulder height — a visible sign of a sideways curve or rotation
- Chronic upper-back muscle fatigue — that deep, end-of-day tiredness between the shoulder blades
The pain rarely comes from the curve itself. It comes from the muscles, joints and discs working under an uneven, sustained load — which is also why the right interventions can reduce symptoms even when the underlying curve doesn't fully straighten. When the small joints along the curve get stiff and irritated, the ache can take on the deep, local character of facet joint syndrome.
For every inch your head drifts forward of your shoulders, the effective load on your neck and upper-back muscles climbs sharply — which is why posture-driven curves are so good at generating fatigue and ache.
Can scoliosis be corrected?
The honest answer depends on the kind of curve. A functional or postural scoliosis — a sideways shift driven by muscle imbalance, a leg-length difference, or a guarding pattern — is highly responsive and can often be substantially reduced or resolved once the underlying cause is addressed. A structural or idiopathic scoliosis, where the vertebrae themselves are rotated and shaped into the curve, is managed rather than "cured."
Age matters too. In an adolescent who is still growing, a structural curve is watched closely and, past certain thresholds, managed with bracing or surgery to limit progression. In an adult, the curve is generally stable, and the work shifts toward mobility, strength, pain control and keeping the spine functioning well around the curve. Correction in the cosmetic sense is rarely the realistic target for structural curves — better movement and less pain almost always are.
Can kyphosis be reversed?
Postural kyphosis — the rounded upper back built from years of forward-flexed sitting and a weak, lengthened back — is the most reversible spinal curve there is. Because the bones are normal and the curve is held there by soft tissue and habit, it responds well to stretching the tight front, strengthening the back, and retraining default posture. Many people see visible change within a few months of consistent work.
Structural kyphosis is a different story. When wedge-shaped vertebrae cause the curve — as in Scheuermann's kyphosis, which develops in the teen years, or the compression-fracture kyphosis of older adults — the bony shape won't be undone by exercise. The aim there is to halt progression, build supporting strength, and reduce the secondary aches. AAOS OrthoInfo covers how the structural and postural forms are told apart.
The evidence-based approach
The goal isn't a cosmetically perfect spine — it is a spine that moves well, loads evenly and doesn't hurt. For flexible, posture-driven curves, that is very achievable. For structural curves, the aim is to maximize mobility, build support and minimize symptoms.
At The Spine Studio, a curvature-focused plan typically combines:
- Precision spinal adjustments to restore motion to the segments that have stiffened within the curve
- Pin & Stretch and soft-tissue work to release the chronically shortened muscles on the concave side of a curve
- Corrective exercise programming — the core of curvature care: strengthening the muscles that hold you upright and retraining your default posture
- Postural and ergonomic coaching to change the daily positions that built and reinforce the curve
What chiropractic care can and can't do for spinal curves
Being clear about scope is part of doing this well. Here is what conservative, in-clinic care does and doesn't change:
- What it can do. Improve posture and the flexible component of a curve, restore segmental motion, calm the muscle and joint pain a curve generates, and build the strength that holds better alignment over time.
- What it co-manages. For moderate structural curves, we work alongside your orthopedist or pediatrician — supporting function and comfort while they monitor the curve's progression.
- What it can't replace. Chiropractic does not substitute for bracing in a growing adolescent or for surgical care in severe structural scoliosis. When a curve crosses those thresholds, referral is the right call, and we make it.
No adjustment straightens a structurally rotated spine, and any provider promising to "cure" structural scoliosis with manipulation alone is overselling. Honest scope is the point.
Exercises and daily habits that help
Small, consistent changes move postural curves the most. A few that earn their place:
- Open the front, strengthen the back. Stretch the chest in a doorway and train rows and prone back extensions to counter a rounding upper back — the simplest, most effective rounded-shoulders fix there is.
- Reset your workstation. Screen at eye level, feet flat, hips slightly above the knees — so neutral posture is the easy default rather than a constant effort.
- Take posture breaks. Every 30 to 45 minutes, stand, roll the shoulders back and lengthen tall. Frequent resets beat occasionally trying to sit up straight.
- Train the side that needs it. For asymmetric curves, targeted single-side strengthening and breathing drills help even out the load — these are prescribed off your assessment, not guessed at.
- Move daily. Walking, swimming and general mobility keep the whole spine supple, which makes every other piece of postural correction work better.
When to get assessed
Get evaluated if you notice a deepening hunch, shoulders or hips that sit unevenly, a rib or shoulder-blade prominence when you bend forward, or upper-back ache that won't settle. For a child or teen, any visible asymmetry during growth is worth checking promptly — that is the window when monitoring matters most.
Whether a curve is structural or postural changes the entire plan, and sorting that out is the first job of a proper exam. At The Spine Studio, a $149 initial assessment measures what is flexible, what is fixed, and where your pain is actually coming from. From there, $60 follow-up visits carry the plan forward — each one includes a precision adjustment plus one soft-tissue modality (Pin & Stretch, Cupping & Scraping, or Corrective Exercise Programming) at no extra charge. For curves that aggravate the low back during lifting, our notes on lifting through low-back pain pair well with a curvature plan.
Whether a curve is structural or postural changes the entire plan — and that is the first thing a proper assessment sorts out. We'll measure what is flexible, what is fixed, and build a program around what can actually change.
Managing kyphosis or scoliosis is part of the care we provide from our Cottleville clinic, serving O'Fallon and St. Charles County.
Get a clear assessment and a realistic plan.
Frequently asked questions
- Can scoliosis be treated without surgery?
- For most mild-to-moderate cases, yes. Surgery is reserved for severe, progressing curves; the great majority are managed conservatively with mobility work, targeted strengthening and posture retraining to reduce pain and slow progression. We assess the curve first and refer on if it needs a specialist.
- Can a chiropractor help with scoliosis?
- A chiropractor can meaningfully reduce the pain, stiffness and muscle imbalance that come with scoliosis, and improve how well you move — but no one straightens an established adult curve by hand. We're honest about that distinction: we treat symptoms and function, not the bony curve itself.
- What is the difference between kyphosis and scoliosis?
- Kyphosis is an exaggerated front-to-back rounding of the upper back (a sagittal-plane curve). Scoliosis is a sideways, often rotated curve of the spine (a coronal-plane curve). They can occur separately or together, and each is assessed and managed differently.
- Is scoliosis pain reversible?
- The pain and movement restriction usually improve a great deal with the right plan, even when the structural curve stays the same. In adults the curve itself is generally managed rather than reversed; the goal is a comfortable, well-functioning spine around it.

