Spinal decompression therapy: how we relieve a pinched nerve.
Most people picture spinal decompression as a motorized table that stretches your spine. Here's what decompression actually means, what the evidence supports, and how we relieve disc and nerve compression the honest way.
Most people who search for spinal decompression are picturing one specific thing: a motorized table that straps you in, stretches the spine, and pulls a bulging disc back into place. That image comes from advertising, and it has crowded out the simpler truth. Decompression is not a machine. It is a goal — taking pressure off a disc or nerve that has too much of it.
When a disc bulges, a joint stiffens, or the bony channel a nerve travels through narrows, the result is the same: a structure that needs space is getting squeezed. Relieving that pressure is the work. The table is one way some clinics attempt it. It is not the only way, and for most patients it is not the most reliable one.
What spinal decompression actually means
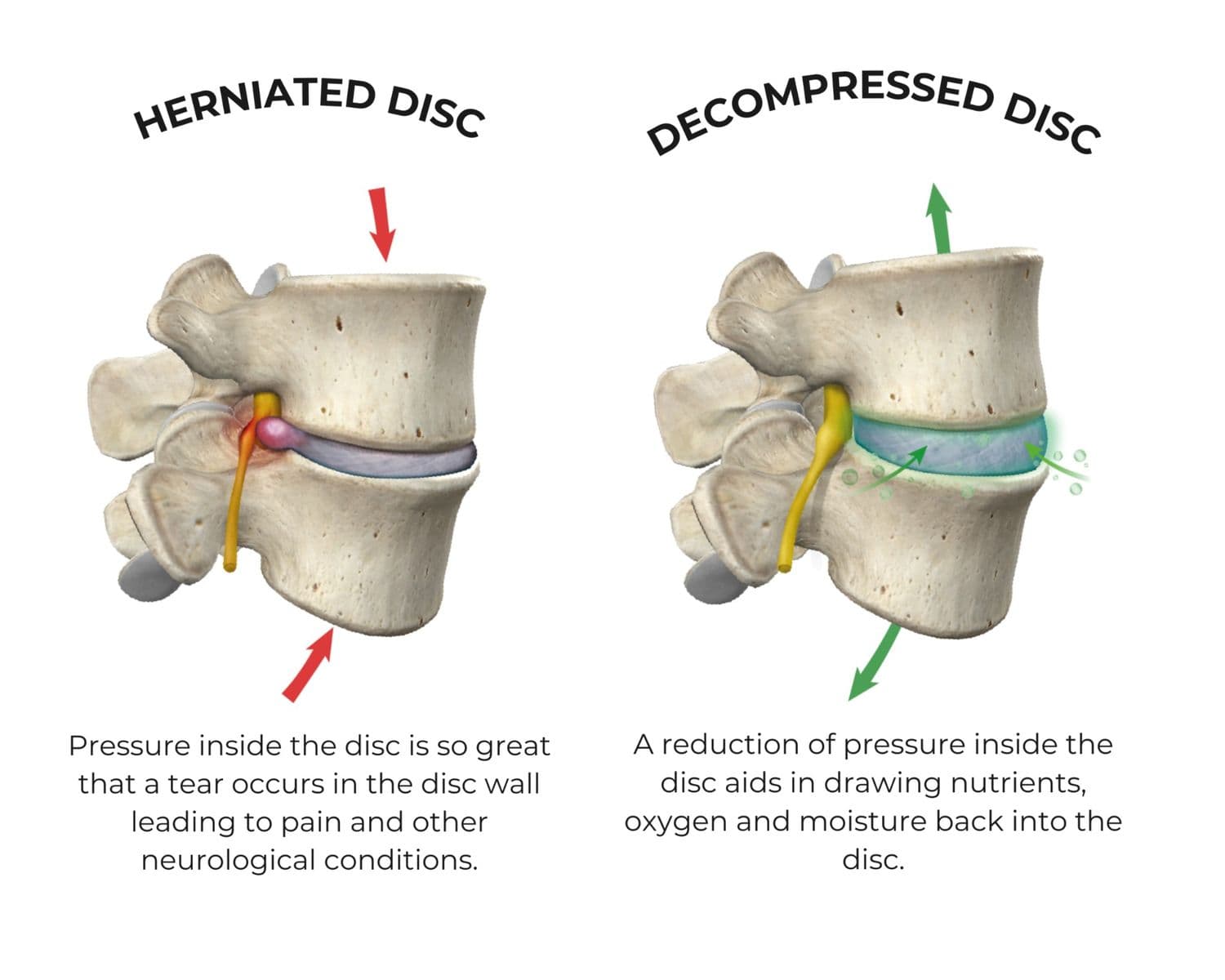
Decompression means reducing the load on a compressed structure in the spine — usually a disc, a nerve root, or both. A healthy disc holds height and acts as a spacer between two vertebrae. When it loses height or bulges backward, the space where the nerve root exits gets tighter, and the nerve starts complaining.
That complaint is what sends people looking for answers. It shows up as sciatica running down the leg, as numbness or tingling in the foot, or as a deep ache that worsens with sitting. The underlying causes are familiar: a lumbar disc herniation pressing on a root, a facet joint that has stiffened and inflamed, or foraminal narrowing where the exit channel has closed down with age.
Decompression is not a product you buy. It is what happens when the structure that was being squeezed finally gets its space back.
The point worth holding onto: the leg pain, the tingling, the stiffness — these are downstream signals. Decompression-style care aims upstream, at whatever is doing the squeezing.
Motorized decompression tables vs. the honest version
Motorized decompression tables are real, and they are marketed heavily. The premise is mechanical: a computerized harness applies cyclical traction to the lumbar or cervical spine, theoretically creating negative pressure inside the disc that draws the bulge inward and pulls in fluid and nutrients.
The evidence is more modest than the advertising. Some patients with disc-related leg pain do report relief from traction-based protocols, but high-quality trials have not shown motorized decompression to be clearly superior to active conservative care, and major reviews treat it as one option among many rather than a breakthrough. The Mayo Clinic frames disc treatment around movement, targeted therapy, and time — not a single machine.
The Spine Studio does not run a motorized traction table, and we are not going to pretend a machine is the only path to taking pressure off a nerve. What we do instead is decompress the spine the honest way: by restoring motion, opening tissue, freeing the nerve, and rebuilding the support that keeps the space open. Manual and active, not motorized.
How we relieve spinal compression at The Spine Studio
Compression has more than one source, so relief has more than one lever. We start every case with an exam to find out which structure is actually being pinched, then build the plan around that finding rather than around a single piece of equipment.
- Precision spinal adjustments. A stiff, jammed segment loads the disc and joint around it unevenly. Restoring normal motion to that segment redistributes load and gives the compressed area room to settle.
- Pin & Stretch. The muscles guarding an irritated level pull the joint tighter and clamp down on the surrounding tissue. Releasing them under active motion lengthens the tissue and reduces the mechanical squeeze on the nerve.
- Nerve mobilization (nerve flossing). When a root is irritated, the nerve can get tethered and tension-sensitive. Gentle, specific gliding moves the nerve through its sheath so it stops catching at the compressed point.
- Corrective exercise. This is the part that actually keeps the space open. Position-specific movements — often spinal extension work for disc-driven cases — plus glute and core strength take chronic load off the disc so it stops being re-compressed every day.
A first visit is a $149 initial assessment. Follow-up visits are $60 and include a precision adjustment plus one soft-tissue modality — Pin & Stretch, Cupping & Scraping, or Corrective Exercise Programming — at no extra charge. Acupuncture, performed by an acupuncture qualified chiropractor, is $60 per session and pairs well with nerve-irritation cases. For stubborn tissue, Shockwave Therapy is offered as a $375 three-session package, the minimum recommended course for tissue repair.
Conditions where decompression-style care helps
Not every back complaint is a compression problem, but a large share are. The cases that respond best to this kind of care share a pattern: something has lost space, and the nerve or disc is paying for it.
- Sciatica. Leg pain driven by a compressed lumbar nerve root — the classic target for taking pressure off and restoring glide.
- Lumbar disc herniation. A bulging or herniated disc crowding the root; adjustments, nerve work, and extension-based exercise are the conservative front line.
- Facet and foraminal narrowing. Age-related closing of the joints and exit channels, common past 45, that responds to restoring motion and offloading the segment.
- Stiff, compressed low backs. The chronically tight, achy spine that feels jammed first thing in the morning and after long sitting — often a motion and load problem more than a structural one.
People who lift are a frequent fit here, because loading a compressed spine the wrong way keeps re-aggravating it. Our notes on lifting through low back pain cover how to keep training while the nerve settles.
Does spinal decompression work?
For the right cases, yes — when "decompression" is understood as the goal rather than a single machine. Conservative care that restores motion, frees the nerve, and rebuilds support has strong evidence behind it for disc-related and nerve-related back pain. Motorized traction tables have weaker, mixed evidence and are best seen as one possible tool, not the deciding factor. What predicts a good outcome is matching the treatment to the actual source of compression, which is why the exam comes before anything else.
Is spinal decompression safe?
Manual and active decompression-style care is safe for the large majority of patients when it follows a proper exam. The exam exists to rule out the cases that need a different path — and a small number do. Progressive weakness, an unrelenting and worsening pain pattern, or the red flags below change the plan entirely. For most people with disc or nerve compression, restoring motion and offloading the spine is both safe and the fastest route back to normal. The AAOS OrthoInfo library is a reliable second reference on conservative disc care.
Sudden numbness in the saddle area between your legs, loss of bowel or bladder control, or rapidly progressing weakness in both legs is a medical emergency called cauda equina syndrome. These signs are rare, but they are surgical. Don't book an appointment — go to the emergency room.
Decompression care near you
If you have been searching for spinal decompression therapy near you — in O'Fallon, St. Peters, or anywhere in St. Charles County — the honest answer is that the right care starts with finding out what is actually being pinched, not with booking time on a machine. From our Cottleville clinic, we serve patients across the area who want their disc and nerve pain handled by an exam-first plan rather than a one-size traction protocol.
If your back is squeezing a nerve, the fastest way out is identifying which structure has lost its space — and then doing the specific work that gives it back.
The Spine Studio treats disc and nerve-compression pain from our Cottleville clinic — serving O'Fallon, St. Peters, St. Charles and the wider St. Charles County area. If you searched for spinal decompression in O'Fallon, that care now happens a short drive down Highway N.
Book an assessment to find what's actually being pinched.
Frequently asked questions
- What is spinal decompression?
- Spinal decompression is any approach that reduces pressure on the discs and nerves of the spine so irritated tissue can settle and rehydrate. At The Spine Studio we achieve it through specific adjustments, Pin & Stretch soft-tissue work, and corrective exercise that restores room and movement to the joint — rather than a single machine.
- Does spinal decompression actually work?
- For the right problem, yes. People with disc-related low-back or neck pain and nerve symptoms often get meaningful relief when pressure is taken off the segment and they restore movement. It is not a cure-all — we assess first and tell you honestly whether decompression-style care is the right fit or whether you need imaging or a referral.
- Where can I get spinal decompression near O'Fallon or Cottleville?
- The Spine Studio is in Cottleville, MO at 5285 State Route N, Suite 102, a few minutes from O'Fallon, St. Peters and St. Charles. We see patients from across St. Charles County for disc and nerve-compression complaints.
- Is spinal decompression the same as a traction table?
- No. A motorized traction table is one tool some clinics use. We don't rely on a traction table — we decompress the segment through hands-on adjustment, Pin & Stretch and loaded corrective exercise, which also addresses why the segment was overloaded in the first place.

