Rotator cuff injury: torn, strained, or just tight?
Shoulder pain reaching overhead or sleeping on your side often gets blamed on 'a torn rotator cuff' — but strain, impingement and an actual tear are three different problems with three different plans.
Reaching overhead. Rolling onto your side at night. Reaching behind your back to grab a seatbelt. When any of these suddenly hurt, "rotator cuff" is usually the first phrase that comes to mind — but strain, impingement, and an actual tear are three genuinely different problems, and telling them apart changes everything about the plan.
Anatomy made simple
The rotator cuff is a group of four small muscles and their tendons that wrap around the shoulder joint, holding the ball of the upper arm bone snugly in its socket while also powering rotation and lifting. Unlike the big, obvious deltoid muscle on top of the shoulder, the rotator cuff does its work quietly, stabilizing the joint through nearly every arm movement you make.
Because these tendons are relatively thin and pass through a tight space under a bony arch, they're vulnerable to three related but distinct problems: a strain (overstretched but intact), impingement (repeatedly pinched under that bony arch), and a tear (partial or full-thickness disruption of the tendon fibers).
How it connects to the Pain Locator
On the Pain Locator, rotator cuff strain sits at the shoulder alongside shoulder impingement, frozen shoulder, and AC joint sprain — four conditions that often get lumped together but have distinct presentations:
- Pain with specific overhead or reaching movements — rather than pain in every direction
- Weakness with resisted movement — a genuine strength deficit, not just discomfort, is the hallmark that separates a more significant tear from a simple strain
- Night pain, especially lying on the affected side — one of the most common complaints regardless of severity
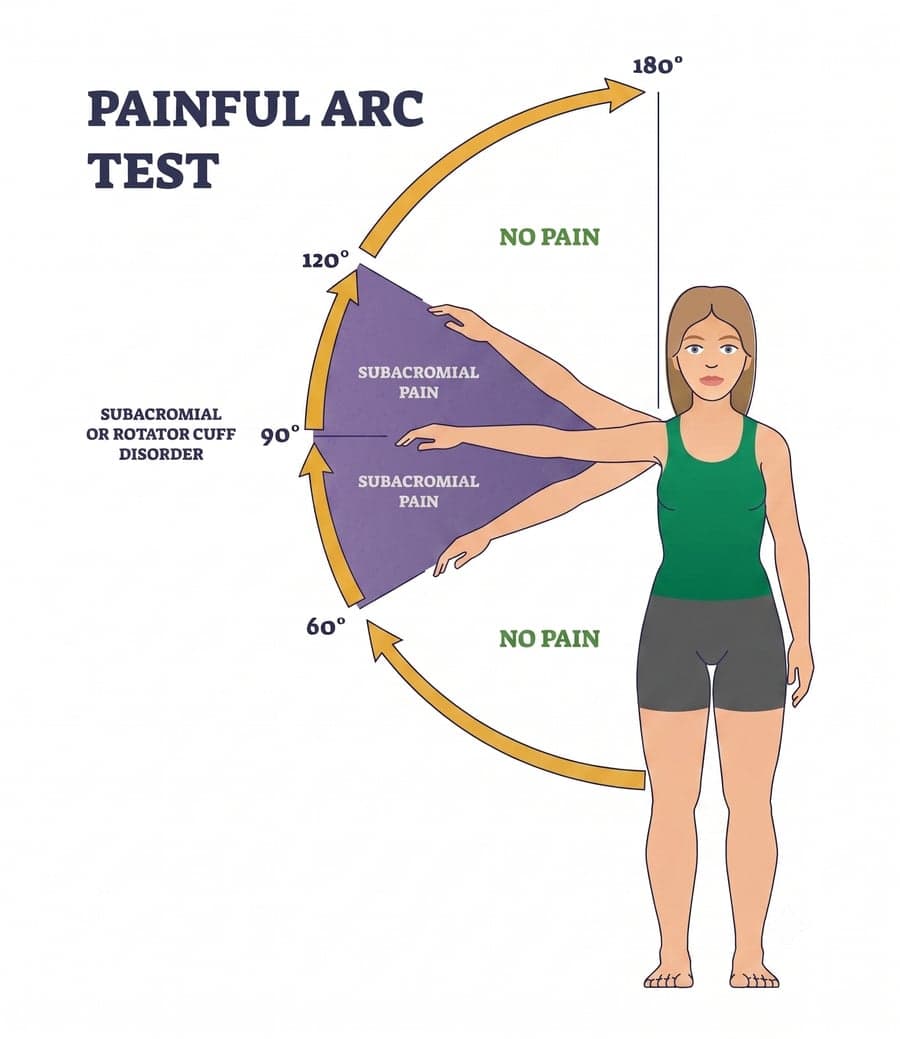
The painful arc test
One of the simplest ways to spot a rotator cuff problem is called the painful arc test: raise your arm out to the side, away from your body, and pay attention to exactly where pain shows up. A positive result has a specific pattern — no pain from 0° to about 60°, pain that kicks in and builds from roughly 60° to 120°, and then pain that eases again as the arm continues overhead toward 180°.
That middle band of pain, between about 60° and 120°, is the giveaway. It's the exact range where the irritated tendon or bursa gets squeezed underneath the bony arch of the shoulder (the acromion) — the same pinching mechanism behind subacromial impingement and rotator cuff-related pain. Pain that's constant through the whole range, or pain that shows up in a completely different pattern, points toward a different cause, like a joint or a frozen-shoulder problem instead.
Rotator cuff vs. frozen shoulder — the key difference
This is the distinction that matters most in the exam room. A rotator cuff problem is about the tendons: painful or weak with specific movements, but someone else can often still move your arm through most of its range even when you can't do it yourself against resistance. Frozen shoulder is about the joint capsule itself contracting, which blocks motion in every direction no matter who's moving the arm — active or passive. That single test, checked properly, usually separates the two before any imaging is needed.
Weakness with resisted movement, not just pain, is the detail that tells a strain from a real tear — and it's the detail people describing their own shoulder pain almost never mention on their own.
The evidence-based approach
Strains, impingement, and many partial tears respond well to conservative care focused on the whole shoulder complex, not just the sore spot:
- Corrective exercise programming targeting the rotator cuff and shoulder blade stabilizers — the single most evidence-supported piece of recovering from cuff-related pain
- Pin & Stretch and soft-tissue work on the surrounding muscles that compensate and tighten around an irritated cuff
- Precision spinal adjustments to the upper back and neck, since restricted mid-back mobility often forces the shoulder to compensate and can worsen impingement
Larger, full-thickness tears — especially in younger or highly active patients — sometimes warrant a surgical opinion, which a proper exam should flag rather than assume either way.
Sleeping on the unaffected side with a pillow supporting the sore arm reduces the direct compression that makes rotator cuff pain classically worse at night, while the underlying issue gets addressed.
An exam at The Spine Studio tests each rotator cuff muscle individually to find out what's actually going on before assuming the worst.
Get a real exam before assuming it's a tear.
Frequently asked questions
- How do I know if I have a rotator cuff tear or just a strain?
- A strain typically causes pain with specific movements but the shoulder still moves through a full range, just uncomfortably. A more significant tear often causes real weakness — an inability to hold the arm up against light resistance, not just pain when you try. An exam that specifically tests each rotator cuff muscle can usually tell the difference without needing an MRI first.
- What is the painful arc test for the shoulder?
- It's a simple self-check: raise your arm out to the side and notice where pain shows up. A positive result — no pain below about 60 degrees, pain that builds between 60 and 120 degrees, then eases again as the arm goes overhead — points to subacromial impingement or a rotator cuff problem, since that middle range is exactly where the irritated tendon gets pinched under the shoulder blade's bony arch.
- What is the difference between rotator cuff injury and frozen shoulder?
- Rotator cuff problems are about the tendons — pain and weakness with specific movements, but the joint can usually still be moved through most of its range by someone else even when it hurts to move actively. Frozen shoulder is about the joint capsule itself contracting, which blocks motion in every direction regardless of who's moving the arm. That distinction is the key thing an exam checks.
- Can a rotator cuff injury heal without surgery?
- Many strains, partial tears and impingement-type injuries improve significantly with conservative care — targeted exercise, soft-tissue work, and addressing the shoulder blade mechanics that often contribute. Larger, full-thickness tears, especially in younger or more active patients, sometimes need a surgical opinion, which a good exam will flag rather than assume.
- Why does my shoulder hurt more at night?
- Rotator cuff irritation is classically worse at night, partly because side-sleeping compresses the shoulder structures directly and partly because there's no daytime movement to keep inflammation from settling into the joint. Side-sleeping on the unaffected shoulder, with a pillow supporting the affected arm, often reduces night pain while the underlying issue is addressed.